Construction Workplace Injury Statistics UK
Construction is consistently the most dangerous major industry in the UK. Year after year, it records the highest number of fatal workplace injuries of any sector, a fatal injury rate nearly five times the national average, and non-fatal injury rates significantly above those of comparable industries — despite decades of regulatory development, enforcement activity, and safety improvement campaigns.
The scale of the challenge is not simply a function of the work being inherently dangerous. Construction sites are dynamic, multi-contractor environments where hazards change daily, where the workforce includes a high proportion of self-employed individuals who may have limited access to formal safety support, and where the pressure of project timelines and costs can create conditions in which risk management is sometimes deprioritised.
This guide brings together the latest verified UK construction workplace injury statistics from the HSE and other authoritative sources, covering fatalities, non-fatal injuries, occupational disease, costs, and what the data shows about prevention.
Key facts & figures (overview)
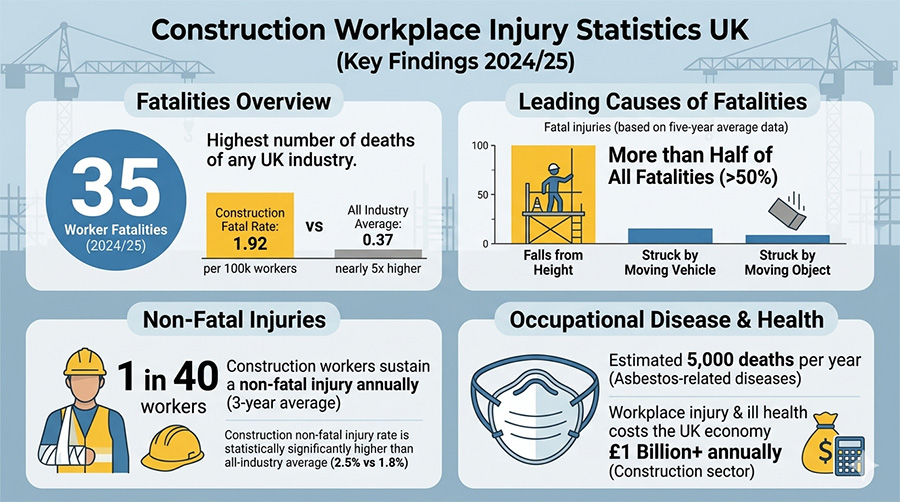
- 35 worker fatalities in construction in 2024/25 — the highest of any industry sector in the UK, accounting for 28% of all worker deaths despite the sector employing just 6% of Great Britain’s workforce.
- 1.92 per 100,000 workers — the construction fatal injury rate, approximately 4.8 times the all-industry average of 0.37.
- ~40 deaths per year — the five-year average for construction fatalities (2020/21–2024/25).
- More than half of all construction fatalities (five-year average) are caused by falls from height — the leading cause.
- 50,000 construction workers self-reported a non-fatal injury over the three-year period 2022/23 to 2024/25 — equivalent to 1 in 40 workers in the sector.
- 2.5% per 100,000 workers — construction’s non-fatal injury rate, statistically significantly higher than the all-industry average of 1.8% and higher than manufacturing (2.1%).
- 33% + 30% — falls from height (33%) and slips, trips and falls (30%) together account for more than half of all non-fatal injuries in the sector.
- 52% of MSDs in construction are linked to manual handling; construction is the leading sector for above-average musculoskeletal disorder rates.
- ~5,000 deaths per year from asbestos-related diseases — construction’s most significant long-term health hazard, predominantly among workers exposed during the sector’s peak asbestos use in the 1950s–1980s.
- 4 members of the public were also killed in construction-related incidents in 2024/25, consistent with the five-year average.
Fatal injuries in UK construction
- In 2024/25, 35 workers were killed in construction-related accidents — the highest of any sector and a figure that represents a significant reduction from the 51 deaths recorded in 2023/24, though still above the five-year average.
- Construction accounts for 28% of all UK workplace fatalities while employing only 6% of the workforce — a disparity that underlines the inherently elevated risk profile of the sector.
- The fatal injury rate of 1.92 per 100,000 workers means that construction workers are approximately 4.8 times more likely to be killed at work than the average UK worker.
- The five-year average of approximately 40 construction deaths per year provides the most statistically reliable benchmark, smoothing out year-on-year variation in the relatively small absolute numbers.
- An additional 4 members of the public were killed in incidents connected to construction activities in 2024/25 — including members of the public on or near construction sites.
- Despite the long-term reduction in construction fatalities — from well over 100 per year in the early 1980s — progress has broadly plateaued over the past decade, with the rate remaining stubbornly above what the evidence suggests is achievable.
The leading causes of construction fatalities
The causes of fatal construction injuries are well established and have changed remarkably little over many decades. Three types of accident together account for the majority of construction deaths every year:
Falls from height remain the single most common cause of death in construction. Over the five-year average, falls from height account for more than half of all construction fatalities — a proportion that has remained broadly consistent since records began. In 2024/25 specifically, falls from height were responsible for 35 fatalities nationally (across all industries), with construction representing the largest share. Scaffolding, roofwork, ladders, edges, and fragile surfaces are the most frequent scenarios. The construction industry accounts for the largest share of the national falls-from-height death toll in nearly every year.
Being struck by a moving object is the second most significant fatal hazard in construction. Falling materials, swinging loads from cranes and lifting equipment, and objects dislodged from height are persistent causes of both fatal and serious injury on construction sites.
Being trapped by something collapsing or overturning — including trench collapses, excavation failures, and the overturning of plant and equipment — contributed to 17 fatalities nationally in 2024/25. Excavation collapse is a particularly acute risk on civil engineering projects.
Being struck by a moving vehicle — particularly on busy construction sites where HGVs, plant, and pedestrians share access routes — remains a significant cause of death. Vehicle-pedestrian segregation on construction sites is a persistent area of regulatory focus.
These four accident types together account for the substantial majority of construction fatalities. They share a common characteristic: all are directly preventable through the application of well-understood engineering controls, safe systems of work, and appropriate training and supervision.
Non-fatal injuries in construction
While fatal injuries attract the most attention, non-fatal injuries represent a far greater volume of harm to construction workers:
- An estimated 50,000 construction workers self-reported sustaining a non-fatal injury over the three-year period from 2022/23 to 2024/25, according to the HSE’s preferred data source, the Labour Force Survey.
- This equates to approximately 1 in 40 workers sustaining a non-fatal injury over that period.
- 29% of these injuries resulted in absence from work of more than seven days — reflecting the severity of many construction injuries compared to other sectors.
- Construction’s non-fatal injury rate of 2.5% per 100,000 workers is statistically significantly above the all-industry average of 1.8%, and above the rates recorded in manufacturing (2.1%) and transportation and storage (1.9%).
- Under RIDDOR (employer-reported figures), construction consistently ranks among the highest-reporting sectors for non-fatal injuries — though, as with all sectors, self-reported figures from the Labour Force Survey are substantially higher than employer-reported figures, indicating significant underreporting.
- Non-fatal construction injuries result in millions of lost working days annually, with substantial productivity, operational, and compensation costs falling on construction businesses of all sizes.
The leading causes of construction non-fatal injuries
RIDDOR data for the period 2022/23 to 2024/25 identifies the following as the most significant causes of non-fatal injuries in construction:
Falls from height: 33% of non-fatal injuries. Falls from height are the leading cause of non-fatal injuries in construction as well as fatalities — though many non-fatal falls are from relatively low heights, they still frequently result in serious fractures, head injuries, and spinal injuries. Ladders, scaffolding, roofs, and fragile surfaces are the most common scenarios.
Slips, trips and falls on the same level: 30% of non-fatal injuries. The most common cause of non-fatal workplace injury nationally is particularly prevalent on construction sites due to uneven ground, mud, debris, cables, and tools left on walking routes. Together with falls from height, these two categories account for more than half of all non-fatal construction injuries.
Manual handling: a significant contributor to both acute injury and cumulative musculoskeletal disorders. Construction workers — particularly in trades involving heavy materials, brickwork, joinery, and groundworks — face exceptionally high manual handling loads throughout their working lives.
Struck by a moving, flying or falling object: tools, materials, and debris falling or being projected are a consistent source of injury, particularly in areas directly below elevated work.
Contact with moving machinery and plant: excavators, compactors, and other construction plant create ongoing risk of contact injuries, particularly when machinery operates near workers on foot.
Construction ill health: the bigger picture
Fatal accidents and non-fatal injuries represent only part of the health burden borne by construction workers. Work-related ill health — developing gradually over years or decades of exposure — is responsible for far more deaths and disability than acute accidents, and is frequently overlooked in safety discussions focused on immediate incident prevention.
Construction is the leading sector for work-related musculoskeletal disorders, with above-average MSD rates consistently identified by HSE data for 2022/23 to 2024/25. Skilled construction trades show among the highest MSD rates of any occupational group.
Construction workers face significant respiratory disease risk from dust, fumes, and chemical exposures inherent in many construction activities — including wood dust, silica dust from cutting stone and concrete, isocyanate paints, welding fumes, and asbestos.
Work-related stress and mental health is an increasingly recognised issue in construction, driven by job insecurity, self-employment, project pressure, and a cultural reluctance to discuss mental health concerns in a sector with a historically macho culture. Construction has one of the highest rates of suicide among male-dominated occupational sectors in the UK — a pattern that is not fully captured in HSE ill health statistics but is well documented in occupational health research.
Asbestos: the biggest killer in construction
The most significant occupational health issue in construction is not falls from height, nor manual handling, nor any of the acute hazards that dominate safety conversations. It is asbestos — and its consequences are still being felt decades after peak exposure periods ended.
- Approximately 5,000 people die every year from asbestos-related diseases in the UK — including mesothelioma, asbestos-related lung cancer, asbestosis, and pleural thickening. The majority of these deaths occur in people who were exposed while working in construction or related trades during the period of widespread asbestos use (1950s–1980s).
- In 2023, 2,218 people died from mesothelioma — a cancer caused almost exclusively by asbestos exposure, with a latency period of 20–50 years between exposure and diagnosis. A similar estimated number die from asbestos-related lung cancer each year.
- Men who worked in the building industry when asbestos was used extensively continue to represent the largest group of mesothelioma victims.
- Annual mesothelioma deaths are projected to continue declining through the 2020s and 2030s as the cohort of heavily exposed workers ages, but deaths among women — many of whom were exposed in office buildings and schools rather than construction — are projected to remain at approximately 400–500 per year for some time.
- Asbestos was banned from use in the UK in 1999, but it remains present in an estimated 300,000 to 500,000 buildings constructed before that date — including schools, hospitals, offices, and housing. Construction workers undertaking refurbishment, maintenance, and demolition work on these buildings face ongoing exposure risk if asbestos-containing materials are not properly identified and managed.
- The Control of Asbestos Regulations 2012 require employers to identify, manage, and control asbestos in buildings they are responsible for, and to ensure that workers who may disturb asbestos during construction or maintenance activities are properly trained and equipped.
Silica dust — a re-emerging risk: Alongside asbestos, silica dust has been identified as a growing occupational health concern in construction. Cutting, grinding, and drilling stone, concrete, brick, and tile generates respirable crystalline silica (RCS) that, when inhaled over sustained periods, causes silicosis, lung cancer, and chronic obstructive pulmonary disease. The HSE has increased enforcement activity targeting RCS exposure in construction, and deaths among relatively young workers in the engineered stone worktop manufacturing sector have prompted specific regulatory action. Construction workers cutting stone cladding, granite surfaces, and concrete structures face significant exposure risk without adequate dust suppression and respiratory protection.
Musculoskeletal disorders in construction
Construction is consistently identified as the sector with the highest rates of work-related MSDs in the UK:
- Construction is the leading industry with above-average MSD rates for the period 2022/23 to 2024/25, according to HSE data.
- 52% of MSDs in construction are directly linked to manual handling — lifting, carrying, pushing, and pulling heavy or awkward materials and equipment.
- Skilled construction trades — bricklayers, groundworkers, joiners, roofers, and scaffolders — perform some of the most physically demanding manual tasks in any sector of the UK economy.
- Back injuries are the most common MSD outcome, followed by upper limb and shoulder conditions from overhead work, repetitive use of hand tools, and sustained awkward postures.
- Vibration-induced conditions — including hand-arm vibration syndrome (HAVS) from the use of power tools, and whole-body vibration from plant operation — are significant additional sources of musculoskeletal harm in construction.
- Construction workers aged 45 and over are disproportionately affected by MSDs, reflecting the accumulated physical burden of decades of demanding manual work — a pattern that contributes to early exit from the industry and places pressure on the availability of experienced tradespeople.
- MSDs in construction result in substantial lost working days, compensation claims, and long-term workforce capacity loss — costs that are particularly acute for smaller contractors who rely heavily on individual skilled workers.
Who is most at risk?
The construction fatality and injury data reveals consistent patterns in who is most exposed to the highest levels of risk:
Self-employed workers are disproportionately represented among construction fatalities. Self-employed individuals make up a substantial portion of the construction workforce — through the industry’s widespread use of subcontracting and labour-only contracts — and typically have less access to formal safety training, supervision, and occupational health support than directly employed workers. The overall fatal injury rate for self-employed workers across all industries is around three times that for employees, and in construction, self-employment is the norm across many trades.
Male workers account for the overwhelming majority of construction fatalities — reflecting the sector’s workforce demographics. In 2025, approximately 1.76 million men were employed in construction compared to around 318,000 women. The concentration of deaths in a male-dominated industry contributes significantly to the gender disparity seen in overall UK workplace fatality statistics.
Older workers face higher fatal and serious injury rates in construction. Workers aged 60 and over account for approximately 40% of all workplace fatalities nationally despite making up only 11–12% of the workforce. In construction, older workers — while often the most experienced — may face age-related changes in balance, strength, and reaction time that increase vulnerability on sites with falls, heavy equipment, and dynamic hazards.
Smaller contractors and subcontractors operate with fewer dedicated health and safety resources, less access to specialist occupational health support, and often under greater time and cost pressure than larger principal contractors. Many serious incidents on construction sites involve smaller subcontractors working within principal contractor-managed projects.
Workers in specialist high-risk trades — including roofers, scaffolders, steel erectors, and groundworkers — face disproportionately elevated risks relative to the construction average, and should be the priority for targeted training and supervision investment.
The cost of construction accidents and ill health
The financial burden of construction accidents and ill health is substantial at every level:
- Construction is among the sectors with the highest rates of both fatal and non-fatal injury, meaning it contributes a disproportionate share of the national £22.9 billion annual cost of workplace injuries and ill health.
- Individual serious construction injuries — particularly those involving spinal damage, traumatic brain injury, or loss of limb — generate the most significant personal injury compensation awards of any occupational sector.
- HSE prosecution fines for construction safety breaches are consistently among the largest handed down in health and safety cases. Under the Sentencing Guidelines, fines for large contractors can run into millions of pounds for cases involving death or serious injury.
- The indirect costs of construction accidents — project delays, programme disruption, reputation damage, loss of tender eligibility, and insurance premium increases — frequently exceed the direct costs of fines and compensation.
- Asbestos-related disease claims represent a substantial and ongoing source of liability for construction companies, building owners, and their insurers — with cases regularly involving exposure that occurred decades before the current management team took responsibility for the business.
- Occupational health costs — including the long-term care and support needs of workers with chronic MSDs, respiratory conditions, and hearing loss — fall on individuals, the NHS, and the welfare system as well as on businesses directly.
Long-term trends
The long-term trend in construction fatalities shows significant improvement followed by a concerning recent plateau:
- Construction fatalities have fallen dramatically over the long term — from well over 150 per year in the early 1980s to the current range of 35–51 per year.
- However, the rate of improvement has broadly stalled over the past decade. The five-year average has remained broadly flat, and the sector has not achieved the sustained reductions seen in earlier periods.
- The 35 deaths in 2024/25 represents a significant improvement on the 51 recorded in 2023/24, but that earlier figure was itself above the five-year average — meaning the positive 2024/25 result should be interpreted as a return to the trend line rather than evidence of a new downward trajectory.
- Non-fatal injury rates in construction have similarly plateaued. While rates are lower than historical figures, no sustained downward trend has been established in recent years.
- Occupational disease mortality — particularly asbestos-related — will continue to generate thousands of deaths per year for the foreseeable future, regardless of current site safety improvements, as a legacy of historical exposures.
- The HSE’s 10-year strategy (2022–2032) does not include a specific numerical target for reducing construction fatalities, but its increased focus on occupational health surveillance and enforcement is particularly relevant to the sector’s dual burden of acute accidents and chronic disease.
How does UK construction compare internationally?
Despite the sector’s poor domestic safety record relative to other UK industries, construction in Great Britain compares reasonably well internationally:
- Great Britain’s overall workplace fatal injury rate of 0.37 per 100,000 workers is among the lowest in Europe, reflecting the impact of decades of regulation and enforcement.
- UK construction’s performance — while significantly worse than the all-industry average — is generally comparable to or better than construction safety records in France, Spain, Italy, and Poland.
- Globally, construction accounts for approximately 30% of all fatal occupational accidents worldwide despite employing around 7% of the global workforce — making the UK sector’s safety challenges part of a universal pattern rather than a UK-specific failure.
- The UK’s relative strength reflects the established regulatory framework, the HSE’s targeted enforcement in construction, and the CDM Regulations 2015 which embed safety into project design and management rather than treating it as a site-level add-on.
Construction’s legal framework
Construction is subject to the most comprehensive occupational safety legal framework of any UK industry sector, reflecting the range and severity of hazards involved:
- The Health and Safety at Work etc. Act 1974 — the foundational duty on all employers, including construction clients, principal contractors, and subcontractors, to ensure health, safety, and welfare so far as is reasonably practicable.
- The Construction (Design and Management) Regulations 2015 (CDM) — the most significant sector-specific legislation, requiring a structured approach to health and safety across the project lifecycle. CDM allocates duties to clients, principal designers, principal contractors, and other duty holders, and requires that safety is considered from the design stage rather than managed reactively on site.
- The Work at Height Regulations 2005 — requiring employers to avoid work at height where possible, use appropriate equipment where it cannot be avoided, and ensure workers are competent and properly supervised. Given that falls from height cause more than half of construction deaths, compliance with these regulations is the single most important legal obligation for most construction businesses.
- The Manual Handling Operations Regulations 1992 — requiring employers to avoid, assess, and reduce manual handling risks across construction tasks.
- The Control of Asbestos Regulations 2012 — requiring employers to manage asbestos in buildings they control and to ensure workers who may disturb asbestos are properly trained (minimum category requirement), appropriately equipped, and supervised.
- The Control of Substances Hazardous to Health Regulations 2002 (COSHH) — covering dust, fumes, chemicals, and biological agents encountered on construction sites, including silica dust, wood dust, welding fumes, and isocyanate paints.
- The Control of Vibration at Work Regulations 2005 — setting exposure limits for hand-arm vibration from power tools and whole-body vibration from plant.
- The Provision and Use of Work Equipment Regulations 1998 (PUWER) — covering all construction plant and equipment.
- RIDDOR 2013 — requiring the reporting of fatal and specified serious injuries to the HSE, with construction among the highest-reporting sectors.
- The Corporate Manslaughter and Corporate Homicide Act 2007 — enabling prosecution of organisations where gross management failure causes death, with unlimited fines and publicity orders available as penalties.
Preventing construction injuries: what works
The hazards that kill and injure construction workers are well understood, and the controls that prevent them are well established. The persistent concentration of deaths in a small number of hazard categories points clearly to where prevention effort must be directed.
Falls from height
- Plan all work at height before it begins — select the most appropriate access equipment for the specific task.
- Use collective protection measures (scaffolding, edge protection, safety nets, air bags) before relying on personal fall protection (harnesses).
- Ensure all temporary works structures — scaffolding, edge protection, working platforms — are erected, altered, and dismantled by trained, competent persons and inspected before use and at regular intervals.
- Prohibit work on fragile surfaces without appropriate access systems and warning systems.
- Brief all workers on height risks during site induction, and reinforce through regular toolbox talks.
Manual handling and MSDs
- Mechanise or eliminate manual handling tasks wherever possible — hoists, material lifts, pallet trucks, and mechanical handling solutions can eliminate many of the highest-risk tasks.
- Provide manual handling training appropriate to the specific tasks performed on site — generic training is insufficient.
- Conduct task-level risk assessments for construction activities involving repeated lifting, carrying, or awkward postures.
- Monitor for early symptoms of MSDs and implement early occupational health intervention before conditions become chronic.
Asbestos
- Ensure all buildings to be disturbed, refurbished, or demolished are assessed for asbestos-containing materials before work begins.
- Maintain a comprehensive and up-to-date asbestos register for all premises under management.
- Ensure all workers who may encounter asbestos during refurbishment or maintenance work hold the appropriate asbestos awareness training as a minimum.
- Never allow work that will disturb asbestos to proceed without appropriate licensed contractor involvement where required.
Silica dust and other respiratory hazards
- Use engineering controls — water suppression, on-tool extraction, enclosed cabs on plant — to reduce dust exposure at source before relying on respiratory protective equipment.
- Ensure RPE is correctly selected, face-fit tested, and worn.
- Implement health surveillance for workers regularly exposed to respiratory hazards — early identification of declining lung function allows intervention before conditions become serious.
Across the site
- Foster a genuine safety culture in which workers feel able to raise concerns, stop unsafe work, and report near misses without fear.
- Ensure site inductions are thorough, site-specific, and conducted properly — not rushed to get workers onto tools.
- Apply CDM duties rigorously — safety built into design and pre-construction planning prevents more incidents than reactive site-level controls.
Written by workplace safety experts
This guide was produced by the team at Manual Handling Training, a UK provider of RoSPA-approved and CPD-accredited online health and safety training. Manual handling is among the leading causes of injury and long-term ill health in the construction sector, and our training is used by construction businesses, principal contractors, and specialist subcontractors across the UK to help workers understand the risks they face every day on site. Because construction safety sits at the heart of what we do, we are well placed to present the latest data clearly for safety professionals, site managers, HR teams, and workers alike.
Sources & references
- Health and Safety Executive (HSE) – Construction Statistics in Great Britain 2025
- HSE – Work-Related Fatal Injuries in Great Britain 2024/25
- HSE – Health and Safety at Work: Summary Statistics for Great Britain 2025
- HSE – Occupational Lung Disease Statistics in Great Britain 2025
- HSE – Asbestos-Related Disease Statistics in Great Britain 2025
- HSE – Work-Related Musculoskeletal Disorders Statistics in Great Britain 2025
- HSE – Construction (Design and Management) Regulations 2015
- HSE – Work at Height Regulations 2005
- HSE – Control of Asbestos Regulations 2012
Make sure your team is trained in safe manual handling.
Explore the Manual Handling Training Course →
Mark writes about workplace health & safety, manual handling and accredited online training for Manual Handling Training, part of Online CPD Academy.