Repetitive Strain Injury Statistics UK
Repetitive strain injury is one of the most commonly discussed occupational health conditions in the UK, yet it is also one of the most frequently misunderstood. RSI is not a single diagnosis — it is an umbrella term covering a range of conditions affecting the muscles, tendons, nerves, and soft tissues of the upper body, caused or worsened by repetitive movements, sustained postures, and overuse.
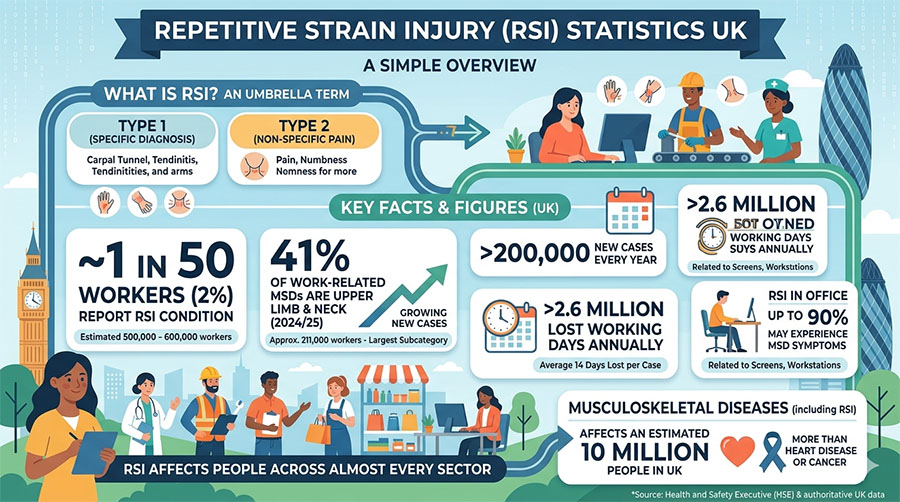
From assembly line workers and keyboard operators to healthcare staff and construction workers, RSI affects people across almost every sector of the UK economy. It is the fastest-growing category within work-related musculoskeletal disorders, driven by both the persistence of physically demanding manual tasks and the rapid expansion of screen-based office work — particularly in hybrid working environments where ergonomic standards are harder to maintain.
This guide brings together the latest verified UK RSI and upper limb disorder statistics from the Health and Safety Executive (HSE), NHS data, and peer-reviewed research, covering prevalence, affected populations, working days lost, costs, and what the evidence shows about prevention.
Key facts & figures (overview)
- 1 in 50 UK workers (2%) reports having an RSI condition — representing an estimated 500,000–600,000 workers at any given time.
- 450,000 UK workers have upper limb RSI specifically affecting the hands, wrists, arms, and neck, according to the Chartered Society of Physiotherapy.
- 200,000+ new cases of work-related upper limb disorders (ULDs) occur in the UK every year, according to the Labour Force Survey.
- 41% of all work-related MSD cases in 2024/25 were upper limb and neck conditions — approximately 211,000 workers.
- 2.6 million+ lost working days per year result from RSI and upper limb disorders, with an average of 14 working days lost per case.
- Up to 90% of office workers may experience MSD symptoms during their careers.
- 10 million people in the UK are affected by musculoskeletal diseases including RSI, carpal tunnel syndrome, and tendinitis — more than those affected by heart disease or cancer.
New cases of upper limb and neck disorders increased between 2023/24 and 2024/25, in contrast to back-related conditions, reflecting growing pressure from repetitive screen-based tasks and hybrid working. Workers in administrative and support service roles have among the highest rates of upper limb MSDs of any occupational group.
What is RSI? Definitions and conditions covered
Before examining the statistics, it is important to understand what RSI does and does not cover — because the term is used differently in different contexts.
RSI (Repetitive Strain Injury) is a lay term, not an official medical diagnosis. In clinical and regulatory settings in the UK, the broader term used is Work-Related Upper Limb Disorder (WRULD) or simply upper limb disorder (ULD). The HSE classifies these conditions as a subset of musculoskeletal disorders (MSDs).
RSI/WRULD is typically divided into two types:
Type 1 RSI
Type 1 RSI is where a specific medical diagnosis can be made, such as:
- Carpal tunnel syndrome (the most common)
- Tendinitis and tenosynovitis
- Tennis elbow (lateral epicondylitis)
- Golfer’s elbow (medial epicondylitis)
- De Quervain’s tenosynovitis
- Rotator cuff syndrome
- Trigger finger
- Vibration white finger / Hand-arm vibration syndrome (HAVS)
- Bursitis
- Writer’s cramp and task-specific focal dystonia
Type 2 RSI
Type 2 RSI is where no specific diagnosis can be made, and the condition is referred to as non-specific upper limb pain or diffuse RSI. This is characterised by pain, numbness, tingling, or cramping without visible swelling or a definitive clinical finding.
Both types are included in HSE statistics on work-related upper limb disorders, and both are covered in this guide.
How many people in the UK have RSI?
Estimating the precise prevalence of RSI in the UK is complicated by the definitional issues noted above — different studies use different case definitions, and many cases go unreported or undiagnosed. However, the available data consistently points to RSI as one of the most common occupational health conditions in the country:
- The HSE estimates that approximately 1 in 50 workers reports RSI symptoms — based on a working population of around 33 million in Great Britain, this suggests roughly 660,000 affected workers at any one time.
- The Chartered Society of Physiotherapy puts the figure at around 450,000 UK workers with upper limb RSI.
- The Business Disability Forum cites one in 50 (half a million) of all workers in the UK as having RSI.
- Musculoskeletal diseases including RSI, carpal tunnel syndrome, and tendinitis collectively affect an estimated 10 million people in the UK — a figure that encompasses both work-related and non-work-related cases.
- Given that upper limb and neck conditions now account for 41% of all work-related MSD cases according to the 2024/25 HSE data — representing approximately 211,000 workers suffering from a condition that was caused or worsened by work — the true occupational burden is substantial and growing.
- These figures are almost certainly underestimates. Many workers do not report symptoms to their employer, do not seek medical attention, or attribute their pain to personal lifestyle factors rather than work. The cumulative and gradual onset of RSI — developing over months or years — means it is frequently not connected to occupational causes until it becomes severe.
RSI and upper limb disorders: the HSE data
The HSE does not publish a standalone RSI figure — RSI conditions are captured within the broader musculoskeletal disorder (MSD) statistics. However, the data on upper limb and neck conditions provides the most direct measure of RSI prevalence in the UK workforce:
- In 2024/25, 511,000 workers were suffering from a work-related MSD. Of these, upper limbs and neck accounted for 41% of cases — approximately 211,000 workers.
- This proportion is growing. Upper limb and neck conditions accounted for 37% of MSD cases in 2023/24; the rise to 41% in 2024/25 represents a significant shift.
- New cases of upper limb and neck disorders increased year-on-year, from approximately 68,000 to over 71,000 new cases, even as back-related new cases held broadly flat.
- Work-related MSDs resulted in 7.1 million lost working days in 2024/25. Applying the 41% upper limb share suggests approximately 2.9 million days lost specifically to upper limb and neck conditions — up from around 2.9 million the previous year.
- The HSE specifically identifies repetitive action and keyboard work as among the three leading self-reported causes of work-related MSDs, alongside manual handling and awkward postures — confirming that RSI risk is not limited to physical industries.
- Workers in administrative and support services, manufacturing, retail, and warehousing show particularly high rates of upper limb MSDs.
Which conditions fall under RSI?
The RSI umbrella covers a range of specific conditions, each with distinct clinical presentations:
Carpal Tunnel Syndrome (CTS) is the most common RSI condition and the most common peripheral nerve entrapment syndrome overall. It is caused by compression of the median nerve as it passes through the carpal tunnel in the wrist, producing tingling, numbness, weakness, and pain in the thumb, index finger, and middle finger. It is particularly prevalent among keyboard workers, assembly line workers, and those using vibrating tools. Research published in BMJ Open tracking UK primary care records found that CTS prevalence increased substantially between 1993 and 2013, driven in part by the growth of computer-based work. Women are disproportionately affected.
Tendinitis and tenosynovitis — inflammation of tendons and their surrounding sheaths — commonly affect the wrists and forearms. Particularly prevalent in assembly, food processing, and repetitive scanning roles.
Tennis elbow (lateral epicondylitis) — pain and tenderness on the outer elbow caused by repetitive overuse of the forearm muscles — affects office workers, keyboard users, and anyone whose work involves repeated gripping, twisting, or lifting actions.
Golfer’s elbow (medial epicondylitis) — similar but affecting the inner elbow — is common in construction, carpentry, and any role involving forceful gripping.
De Quervain’s tenosynovitis — affecting the tendons in the thumb and wrist — is increasingly reported among workers whose roles involve sustained thumb use, including scanning and handheld device operation.
Rotator cuff syndrome — affecting the shoulder — is common in jobs requiring sustained overhead work, reaching, or arm elevation.
Hand-arm vibration syndrome (HAVS) — caused by prolonged use of vibrating tools — produces tingling, whitening of the fingers, and in severe cases, permanent nerve and blood vessel damage. Construction workers, quarry workers, and those using power tools are most at risk. HAVS is a legally reportable occupational disease under RIDDOR.
Diffuse RSI (Type 2) — non-specific pain in the upper limbs without a specific diagnosis — is particularly prevalent among keyboard workers and is often associated with poor workstation setup, extended hours, and inadequate rest breaks.
Working days lost to RSI and upper limb disorders
The productivity impact of RSI on UK workplaces is significant:
- The HSE estimated that 2.6 million working days were lost specifically to upper limb disorders in 2017/18, with an average of 14 days lost per case.
- More recent data from 2024/25 shows that upper limb and neck conditions account for approximately 41% of all MSD-related lost days — equating to roughly 2.9 million working days lost from this category in the most recent year.
- Across all work-related MSDs, 7.1 million working days were lost in 2024/25 — making MSDs, of which RSI is a major component, the second-largest cause of work-related absence after stress.
- The average worker affected by an upper limb disorder loses approximately 14 working days per case, though severe conditions — including carpal tunnel syndrome requiring surgery — can result in significantly longer absences.
- Recovery time after carpal tunnel release surgery averages 21 days for non-manual workers and 39 days for manual workers before return to work, according to research cited in occupational medicine literature.
- These figures capture only formal absence. Many RSI sufferers continue working while in pain — a form of presenteeism that reduces productivity without registering in absence statistics.
Which jobs and industries have the highest RSI rates?
RSI affects workers across many different environments. The HSE and occupational health research identify the following groups as particularly high-risk:
Office and administrative workers — keyboard operators, data entry staff, call centre workers, and anyone using display screen equipment for extended periods. Administrative and support service workers have among the highest rates of work-related upper limb MSDs of any occupational group. The combination of repetitive keyboard and mouse use, sustained static postures, and often inadequate workstation setup creates a high-risk environment.
Assembly line and manufacturing workers — repetitive hand and wrist movements in production, packaging, and quality control roles place significant cumulative strain on the upper limbs. Manufacturing workers face among the highest rates of ULDs per 100,000 workers.
Food processing workers — repetitive cutting, sorting, and packing at speed creates extremely high rates of upper limb RSI. Poultry and meat processing are among the highest-risk specific tasks identified by occupational health research.
Healthcare workers — nursing, care work, and laboratory technicians all involve repetitive fine motor tasks and patient handling that contribute to upper limb strain.
Retail and warehousing — repetitive scanning, reaching, and stock handling create cumulative strain on the upper limbs, shoulders, and neck.
Construction workers — particularly those using vibrating tools (grinders, drills, jackhammers), who face risk of hand-arm vibration syndrome alongside other upper limb conditions.
Cleaning and catering — repetitive wringing, scrubbing, and food preparation activities are consistently identified as high-risk tasks for tenosynovitis and tendinitis.
Other at-risk groups include sign language interpreters, musicians, armed forces personnel, textile and garment workers, and electronics and telecommunications workers.
RSI and office workers: a growing problem
RSI is frequently associated with physically demanding manual work, but office-based workers represent a large and growing share of those affected — and one that is often underserved by traditional workplace health programmes:
- Studies suggest that up to 90% of office workers will experience MSD symptoms at some point during their careers.
- Keyboard and mouse use is one of the most commonly identified causes of work-related upper limb disorders, particularly when workstations are poorly configured or workers use equipment for extended periods without adequate breaks.
- The HSE’s Health and Safety (Display Screen Equipment) Regulations 1992 require employers to assess DSE workstations for all habitual users — yet many employers remain non-compliant, particularly for workers using laptops or working at home.
- Common RSI conditions among office workers include carpal tunnel syndrome, diffuse wrist and forearm pain, tennis elbow from mouse use, and neck and shoulder strain from sustained screen posture.
- Women are significantly more affected than men by office-related RSI, partly because women are more likely to work in administrative roles and are anatomically more susceptible to certain conditions, particularly carpal tunnel syndrome.
- Workers in large organisations (83%) are more likely to report experiencing work-related stress, but small workplaces often have lower rates of formal DSE assessment and ergonomic support, leaving workers equally or more exposed.
Hybrid working and the new RSI risk
The shift to hybrid working has created a new and growing driver of RSI that existing workplace health frameworks were not designed to address:
- Millions of UK workers now routinely work from home using laptop computers on dining tables, sofas, or makeshift desks — environments that fail to meet the ergonomic standards of a properly assessed office workstation.
- The HSE’s DSE Regulations require employers to assess workstations for habitual users — this duty extends to home working environments, but many employers have not formally assessed their remote workers’ home setups.
- Upper limb and neck conditions showed the largest proportional increase of any MSD category in the 2024/25 HSE data, with new cases rising from approximately 68,000 to 71,000 — a trend that occupational health specialists directly link to the deterioration of workstation ergonomics in hybrid and remote working arrangements.
- Studies estimate that up to 90% of office workers will experience MSD symptoms during their careers, and the shift to home working is widening the gap between exposure to ergonomic risk and access to ergonomic support.
- Workers who shift to using laptops without external keyboards, mice, or monitors — even temporarily — quickly adopt postures that place the neck, shoulders, and wrists under sustained strain that accumulates into RSI conditions over weeks and months.
Who is most affected?
RSI does not affect all workers equally. Several demographic and occupational factors consistently appear in the data:
Gender: Women are disproportionately affected by RSI, particularly carpal tunnel syndrome. Women account for approximately 55% of all RSI sufferers according to research on upper limb disorders, partly reflecting their concentration in high-risk administrative, healthcare, and food processing roles, and partly reflecting anatomical differences in the carpal tunnel structure.
Age: RSI can develop at any working age. Approximately one in three workers with RSI is under 45 — a notably high proportion given that age-related degeneration is not yet a factor. RSI is increasingly common among younger workers in their 20s and 30s in screen-based roles. That said, cumulative exposure means risk increases with years of repetitive activity, and older workers in physical roles carry high long-standing condition rates.
Occupation: Workers in administrative, food processing, manufacturing, assembly, and healthcare roles are consistently among the highest-risk groups. Construction workers using vibrating tools face specific risk of HAVS in addition to other upper limb conditions.
Workplace size: Workers in smaller workplaces are less likely to have access to formal DSE assessments, occupational health support, or ergonomic equipment — potentially exposing them to higher cumulative risk despite lower headline injury rates.
The cost of RSI to UK businesses
The financial case for investing in RSI prevention is compelling:
- Work-related upper limb disorders caused approximately 2.6 million lost working days in the most recent specific estimate, at an average of 14 days per case — costs that fall directly on employers through sick pay, reduced productivity, and replacement staffing.
- Across all work-related MSDs, of which upper limb disorders represent the fastest-growing component, the total cost to UK businesses is estimated at £3.5 billion per year in lost productivity, compensation, and healthcare costs.
- Carpal tunnel syndrome surgery — one of the most common treatments for advanced RSI — results in average return-to-work periods of 21 days for non-manual workers and up to 39 days for manual workers, imposing significant operational disruption.
- Compensation claims for RSI arising from employer negligence are well established in UK employment law. Workers have three years from the date of injury (or the date they became aware of the work connection) to bring a personal injury claim.
- Research suggests that for every £1 invested in ergonomic workplace interventions, organisations receive a return of approximately £17.80 through reduced absence, improved productivity, and lower compensation costs.
- Indirect costs — including management time, the impact on team productivity, recruitment and retraining — substantially exceed the direct costs of absence alone.
RSI and the law: employer duties
Employers in the UK have clear legal duties to prevent RSI. Key legislation includes:
- The Health and Safety at Work etc. Act 1974 — places a general duty on employers to ensure, so far as is reasonably practicable, the health, safety, and welfare of all employees, encompassing RSI risk.
- The Management of Health and Safety at Work Regulations 1999 — require employers to conduct suitable risk assessments, including for repetitive tasks and upper limb disorder risks.
- The Health and Safety (Display Screen Equipment) Regulations 1992 — require employers to assess DSE workstations for all habitual users, including home workers, and provide appropriate equipment, training, and eye test entitlements.
- The Manual Handling Operations Regulations 1992 — apply to manual handling tasks that contribute to upper limb MSDs alongside back injuries.
- The Control of Vibration at Work Regulations 2005 — set daily exposure limits for hand-arm vibration, a major cause of HAVS and other upper limb conditions in construction and manufacturing.
- RIDDOR 2013 — requires employers to report certain occupational diseases, including carpal tunnel syndrome caused by work with vibrating tools and tenosynovitis of the hand or forearm caused by repetitive work.
Employers who fail to assess and control RSI risks face HSE enforcement action, and workers who develop RSI through employer negligence have an established route to personal injury compensation.
Preventing RSI: what the evidence shows
RSI is largely preventable. The evidence consistently points to the same set of effective interventions:
For employers
- Conduct DSE assessments for all habitual display screen users — including home and hybrid workers. Many RSI cases among office workers are directly attributable to poorly configured workstations that were never formally assessed.
- Provide appropriate equipment — ergonomic keyboards, mice, chairs, monitor stands, and wrist supports. Equipment choices directly influence posture and strain patterns.
- Implement task rotation and rest breaks — reducing the duration of any single repetitive task is one of the most effective interventions for cumulative upper limb strain. Regular short breaks are more effective than fewer longer breaks.
- Design out repetitive risk where possible — automation, jigs, tools, and process redesign can eliminate the need for high-repetition manual tasks in manufacturing and production environments.
- Train workers and managers to recognise early symptoms of RSI and understand the importance of early reporting. Conditions caught early are far easier to manage.
- Conduct health surveillance for workers in high-risk roles involving vibrating tools — HAVS progression is largely preventable with appropriate monitoring and early withdrawal from exposure.
- Extend ergonomic standards to home workers — provide guidance on home workstation setup, offer equipment loans or allowances, and conduct remote DSE assessments for all habitual home workers.
For workers
- Set up your workstation correctly — screen at eye level, keyboard and mouse at elbow height, back supported, feet flat on the floor.
- Take regular short breaks from repetitive tasks — stand up, move, and stretch every 30–45 minutes.
- Report pain, tingling, or numbness early — do not wait for symptoms to become severe.
- Use ergonomic equipment provided by your employer, and ask for an assessment if none has been offered.
- Avoid using laptops on their own for extended periods — use an external keyboard and mouse whenever possible.
- Maintain general physical activity — strong, well-conditioned muscles are more resistant to repetitive strain.
Written by workplace safety experts
This guide was produced by the team at Manual Handling Training, a UK provider of RoSPA-approved and CPD-accredited online health and safety training. While our core specialism is manual handling, RSI and upper limb disorders develop in the same workplaces, affect the same workers, and are prevented through the same culture of risk awareness and early intervention that underlies all effective workplace health practice.
Sources & references
- Health and Safety Executive (HSE) – Work-Related Musculoskeletal Disorders Statistics in Great Britain 2025
- Health and Safety Executive (HSE) – Health and Safety at Work: Summary Statistics for Great Britain 2025
- HSE – Work-Related Upper Limb Disorders (WRULD) Guidance
- HSE – Health and Safety (Display Screen Equipment) Regulations 1992
- HSE – Control of Vibration at Work Regulations 2005
- AbilityNet – RSI in the Workplace
- Business Disability Forum – Briefing: Employment Adjustments for People with Upper Limb Disorders
- Burton et al. (2018) – Trends in the Prevalence, Incidence and Surgical Management of Carpal Tunnel Syndrome Between 1993 and 2013. BMJ Open
Related guides
Make sure your team is trained in safe manual handling.
Explore the Manual Handling Training Course →
Mark writes about workplace health & safety, manual handling and accredited online training for Manual Handling Training, part of Online CPD Academy.